33247
Views & Citations32247
Likes & Shares
Introduction: Health education
is an essential element, which aims to promote, organize and guide the public
on what to do to maintain optimal health in the third stage of life.
Objective: Identify the level
of knowledge about oral health of older adults.
Method: A descriptive
study of transversal cut was made in the period from January to March 2018 to
44 seniors belonging to the grandparents' house belonging to the joyful hearts
Policlinico Universitario "Salvador Allende, located in the municipality
Boyeros, Havana. He applied a survey on oral health for the elderly age, sex,
level of education, use and care of the prosthesis causes of tooth loss,
knowledge on preventive measures of oral diseases, toxic habits and oral
self-examination, where the following variables were analyzed.
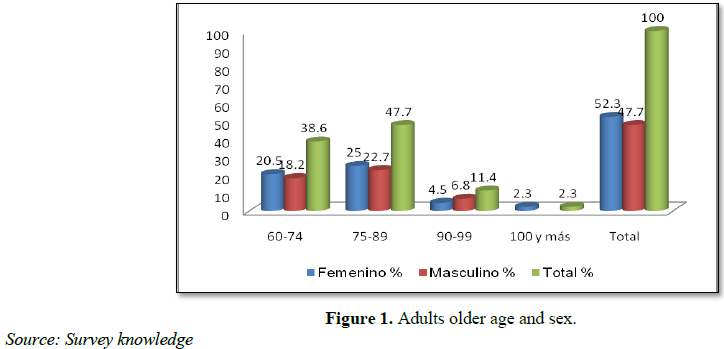
Results: The group of 75 to
89 years predominated with 47.7%, 52.3% of seniors were female and secondary
prevailed with 29.5%. A predominance of knowledge concerning the level of low
level (66%) was identified.
Conclusion: Predominant group
of 75 to 89 years of age, female gender and secondary school, there is a low
level of skills in older adults who participated in the research.
Keywords: Elderly, Prosthetics, Oral cancer, Knowledge
level
INTRODUCTION
Aging is one of the few features that unifies and defines all human
beings. It is considered a universal phenomenon, a dynamic, irreversible,
inevitable and progressive process, in which multiple factors: biological,
psychological and social that involves a number of physiological changes that
influence the function of the organism as a whole, considered by some authors'
an error of the genetic code [1-3].
It defined as the progressive increase in the proportion of elderly in
a given population. In recent decades the analysis of demographic changes over
60 years reflects a fact of great importance, the increase in number of those
aged 80-85 years as a result of increased life expectancy. Due to current
demographic changes, the number of individuals in the world beyond the barrier
of 60 years increased from 400 million people in the decade of the 50 to 700
million people in the 90s of last century and it is forecast to around 1200
million elderly exist in 2025 [4-6].
Educate seniors to promote and protect the health, knowing the risk
factors for the major oral diseases, will be the goal to be achieved by the
model of dental care that responds to the concept of Integral General
Stomatology (EGI), places man as a bio-psycho-social being on different factors
that influence risk, such as attributes that can act negatively on the
occurrence, development and perpetuation of enfermedades [9,10].
Consider that with age becomes more difficult to obtain new knowledge
and learn new practices and behavior change is slower, although we associate
with the psychological, physical status and quality of life. Therefore,
recovery, health maintenance and function of the oral cavity in the elderly
affects significantly their quality of life and the responsibility does not lie
solely in the hands of the dental profession, but in all healthcare and society
and particularly in all families within which there is some adult greater [11].
Health education is a distinctive field in the transmission of
knowledge and the development of a strategy for the conservation of health of
the individual, collective behavior and society [9].
For all the raised and the lack of previous studies in the territory,
it was determined this research in order to identify the level of knowledge on
oral health of seniors in the House of grandparents happy hearts.
METHODOLOGICAL DESIGN
A descriptive study of cross section to the elderly population
attending the grandparents' house belonging to the joyful hearts Policlinico Universitario
Salvador Allende, located in the municipality Boyeros, Havana was conducted.
The study period was from January to March 2018. The population consisted of 44
adults of both sexes belonging to the institution.
To achieve the objectives the survey of knowledge of The National
Program of Stomatology Health [9], the following variables was applied,
modified according to the objectives which were analyzed and operationalized:
·
Age: 60-74, 75-89 and 90-99, 100 and more as the years met.
·
Sex: As biological group (female and male).
· Level schooling: Taking into account the last level up, except the
primary.
The survey addresses on five aspects:
1.
Knowledge use
and care of the dental prosthesis.
2.
Knowledge
about causes of tooth loss.
3.
Knowledge
about preventive measures of oral diseases.
4.
Knowledge of
toxic habits.
5.
The knowledge
of oral self.
To each of whom it was given a score that
allowed quantitatively evaluating the survey in its entirety.
ETHICAL CONSIDERATIONS
Each individual in what was the
investigation, only one oral examination to detect diseases or lesions of the
oral cavity, without invasive procedures and with all the requirements of
hygiene and sterilization of the instrument would be conducted was explained in
detail. He insisted that his participation would be completely voluntary,
without detriment to the relationship with health personnel as a result of
refusal to participate.
The investigation rigorously followed the
ethical precepts for research and design related research, the procedures of
good practice and care data (anonymity, confidentiality and security), in line
with the provisions for epidemiological investigations.
RESULTS
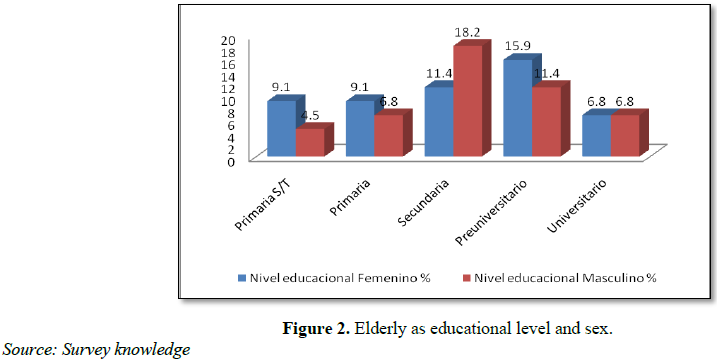
Older adults
studied as educational level and sex is shown in Figure 2. There was a
predominance of basic secondary patients (29.6%), followed by pre-university
(27.3%). No significant relation between the level of schooling and sex found.
In Table 1 the knowledge on oral
health-related criteria shown. On the use and care of dental prostheses of all
older adults studied 72.7% had incorrect knowledge about this. As for knowledge
of causes of tooth loss and the preventive measures of oral diseases they possessed
65.9% and 70.5% respectively incorrect assessment.
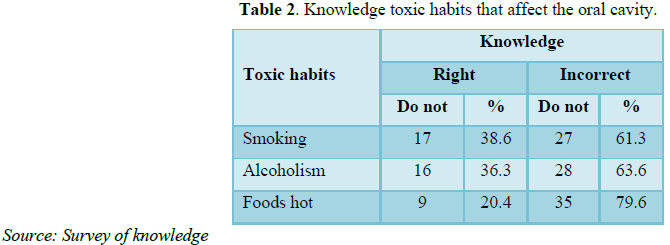
Table 2 presents knowledge of toxic habits that affect the oral cavity is
reflected. It was observed concerning the knowledge of consumption of hot
meals, the highest percentage (79.6%) of incorrect answers. Mientars the
incorrect level of knowledge regarding the toxic alcohol and smoking habits had
a similar behavior with 61.3 and 63.6%, respectively.
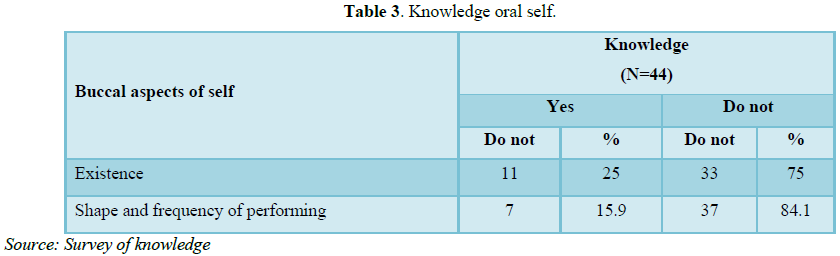
In Table 3 the knowledge about the
existence of oral self-examination is observed. 75% of seniors were unaware of
their existence, 84.1% did not have adequate knowledge of the manner and
frequency in which the same should be done.
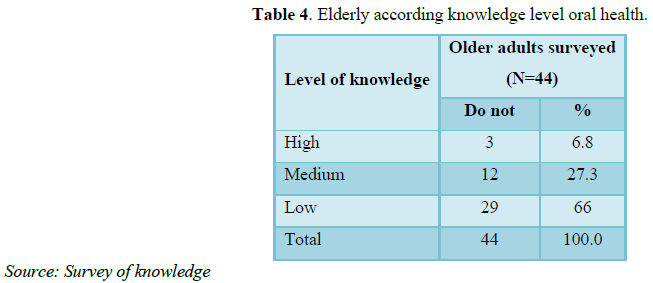
Table 4 shows the level of knowledge about oral health of older adults studied
in the overall assessment, the prevailing low level of knowledge with 66% of
the sample.
DISCUSSION
The aging population is considered, rightly,
one of the great challenges for humanity in the twenty-first century [12,13].
Seniors shown in Figure 1 by age and sex, the same can be seen that the
prevailing age group was 75 to 89 years and on sex predominated feminine.
The above results agree with those obtained by Lima et al. [13] in Brazil in terms of age group and sex. On the other hand there were also matches the results of Ordaz Hernández et al. [14] in the city of Pinar del Río respect to age group, but it was not about sex where men predominated.
Cuba sex behaves as in the rest of the world,
predominantly male births. These are subsequently affected by other conditions
such as excess mortality, which brings with it, which predominates in advanced
age females or that women get to live longer than men. Situation occurring
product given physiological differences between them and the roles they assume
in society, among many other aspects [12,15,16].
As for the educational level of the elderly
and sex (Figure 2); the results of this research are consistent with
those reported in Taiwan by Yen et al. [17], predominating in both the
secondary and differ with studies by Moreno et al. [18] at the University of
Antioquia and Carneiro et al. [19] in Brazil, where predominated the primary
educational level or a low level of schooling.
Taboada Aranza et al. [20] in the work
entitled “Oral Health profile in a group of Hidalgo State Aging” a predominance
of primary level was found (until sixth year of instruction), no matching
results with the present study.
Table 1 shows some related oral health
criteria. Lajes et al. [21] reported in their work there knowledge in a general
sense by seniors about the use and care of dental prostheses; differing results
with those obtained by the author. The final report of the investigation
conducted in the province of Holguin by Romero et al. [22] matches this study.
On issues concerning the cause of tooth loss
or preventive measures of oral diseases results are consistent with research
reports conducted by Martínez Pérez et al. [23] entitled Educational
intervention on oral health club Senior Citizens United for Health and Barrio
Pedraza et al. [24] in the city of Cienfuegos.
Upon analysis of the results obtained with
respect to knowledge of toxic habits that affect the oral cavity it was found
in all cases more than 60% of the sample had incorrect knowledge.
Results that correspond to the high presence
of toxic habits in the elderly population, is consistent with that reported by
Marin Páez et al. [25] at the Polyclinic “Dr. Tomas Romay” Havana. In the city
of Pinar del Rio Dr. Paredes Diaz et al. [26] reported on his research a high
influence of smoking and alcoholism in the health of Pinar del Rio population,
which is related to the results obtained on the low awareness of the damage
causing toxic habits.
In recent years, it has increased the
incidence and mortality from oral cancer. The increased morbidity and
mortality, sequelae of operations and the cost of treatments have led some
countries projected regional programs to detect lesions as early possible [27].
In Cuba Dr. Santana Garay [28] designed the
Program of Oral Cancer Early Detection, which describes the development of
self-oral examination. It is the responsibility of the dentist performing
active investigations to detect lesions of the oral cavity in early stages,
teach patients how to perform oral self-examination.
The results coincide with those set by
Mendoza Fernandez et al. [29] and Rodríguez González et al. [30], both reported
that the population had inadequate knowledge on oral self-examination.
Table 4 reveals it overall assessment of the level of knowledge about oral
health of older adults studied. Predominated the level of knowledge on oral
health, which coincided with the results achieved by Lauzardo et al. [31],
similarly behaved obtained in Mexico by Rodriguez et al. [32].
CONCLUSION
·
Predominant
age group 75 to 89 years, female gender and education level of secondary
school.
·
There was a
predominance of levels of knowledge about oral health of the elderly low.
1. Bayarre HD (2017) Multiple perspectives for
the analysis of demographic aging. A necessity in today's health care
environment. Rev Cuban Public Health 43: 313-316.
2. Rodriguez JR, Tabares VZ, Jiménez ES, López
RS, Del Carmen Cervante Ramos M (2014) Comprehensive geriatric assessment,
importance, advantages and benefits in the management of the elderly. Panorama
Cuba and Health 9: 35-41.
3. Gonzalez LMF, Restrepo GDE, Rovira APT,
Ceballos MV, Gil DLC (2011) Description of clinical oral mucosal changes in
older adults. Natl J Dent 7: 28-34.
4. Arango DC, Peláez E (2012) Population aging
in the twenty-first century. Opportunities, challenges and concerns. Uninorte
Health 28: 335-348.
5. Montero I, Bedmar M (2010) Leisure, free time
and volunteer elderly. Polis Internet 9: 16.
6. Padilla LMS, Pérez UG, González AA, Gallestey
JB (2014) Psychological quality of psychic life and physical health status in
the elderly. Rev haban cienc méd 13: 337-349.
7. Pérez BL, Legrá SMM, Suarez LP, Almestoy LC
(2013) Mouth diseases in the elderly. CCM 17: 477-488.
8. Fuentes MR, Peña YA, López IBH (2016)
Self-perception of oral health in elderly patients with dental prosthesis. Rev
haban cienc méd 15: 210-221.
9. Cuba MINSAP (2011) National Program of
comprehensive dental care to the population. Educational program for a group of
Senior Citizens. Campaign for Dental Health Education (CESD). Havana: Editorial
Medical Sciences, pp: 150-262.
10. González GN, del Castillo EMM (2013) General integral
stomatology. Havana Medical Sciences, p: 359.
11. Alvarez Lauzarique ME, Rocha Rosabal M,
Bayarre See HD, Almenares Hernandez K (2014) Quality of care for the elderly in
the physician of the family. Cubana Med Rev Gen Integr 30: 388-401.
12. Cuba MINSAP (2016) Ministry of Public Health.
National Directorate of Medical Records and Health Statistics. Health
Statistical Yearbook. Havana. Available at: http://bvscuba.sld.cu/anuario-estadistico-de-cuba/
13. Gonzalez R, Cardentey J (2015) Population
aging: A challenge for health professionals in Cuba. Rev Haban Cienc Méd 14:
887-889.
14. Lima I, Pinho HH, Caracterização K (2012)
Correia da Saude mouth of Permanence longa instituiçãobeneficente idososemuma
of Joao Pessoa-PB, Brazil. Rev Cubana Estomatol 49: 193-203.
15. Ordaz Hernández E, Ordaz Hernandez M,
Rodriguez Perera EZ (2015) Oral health in geriatric population: Experience in a
grandparents' house. Rev Med Sci 19: 423-432.
16. Miranda MA (2016) Perspective of the aging in
Cuba. AMC 20: 228-230.
17. Miranda J (2012) Tarragó oral health and
healthy aging. Rev Cubana Estomatol 49: 88.
18. Yen YY, Lee HE Wu YM, Lan SJ, Wang WC, JK Du,
et al. (2015) Impact of removable dentures on oral health-related quality of
life in adults elderly Among Taiwan. BMC Oral Health 15: 1.
19. Moreno JA, Montoya AF, Gomez DP, Grove A, Zea
FJ, et al. (2012) Oral health situation and status edentadobimaxilar prosthetic
patient who comes to the Faculty of Dentistry at the University of Antioquia: A
pilot study. Rev Fac Odontol Univ Antioq 24: 22-36.
20. Carneiro Leao GM, Jorge Moysés S, Moysés Tetu
S, Olandoski M, Anselmo Olinto MT, et al. (2015) Social, economic and
behavioral variables associated with oral health-related quality of life among Brazilian
adults. Ciência Saúde Coletiva 20: 1531-1540.
21. Aranza OT, Colonel XC, Palacio RDH (2014)
Profile of oral health in a group of seniors from Hidalgo State. Revista ADM
71: 77-82.
22. Ugarte ML, López JA, Ramirez SMF, Hidalgo SH
(2014) Breach of prosthetic rehabilitation post signs and their influence on
quality of life. Rev Hum Med 14: 32-47.
23. Junquera CRR, Rodríguez BG, Ortega SG (2015)
Prosthodontics state and oral health status in patients who applied prosthetic
repairs. CCM 19: 38-50.
24. Pérez Martínez ML, Santos Legrá M, Ayala
Pérez Y, Rodríguez Ramos I (2016) Educational intervention on oral health in
the elderly club united for health. CCM 20: 692-701.
25. de Jesus Barrio Pedraza T, Delgado NS,
Neighbourhood EVP, Betancourt AMQ (2009) Educational intervention program for
oral health in the elderly. MediSur 7: 1-6.
26. Marin Páez W, Loyola Veiga L, Reyes Revilla
Y, Mesa González DL (2017) Oral lesions in older adults and risk factors.
Polyclinic “Dr. Tomas Romay”, Havana, Cuba. Rev Haban Cienc Méd 16: 770-783.
27. Diaz Paredes R, Orraca Castillo O, Torres
Marimón ER, Casanova Moreno MC, Martinez D, et al. (2015) Influence of smoking
and alcoholism in the state of health of the population. Pinar Rev Med 19:
46-55.
28. Rodriguez E, Santana KA, Jacas MJ, Quevedo K
(2014) Evaluation program for early detection of oral cancer. AMC 18: 642-655.
29. Santana Garay JC (2002) Prevention and
diagnosis of cancer. Havana: Editorial Medical Sciences, pp: 38-45, 59.
30. Fernández MM, Gonzalez AMO, del Carmen Abreu
Noroña A, Perez OR, Mena MG (2013) Educational intervention for the prevention
of oral cancer in older adults. Rev Med Sci 17: 24-32.
31. González GMR, Gonzalez CFV, Suárez HFC,
Morales DV (2017) Knowledge about oral cancer in a sector of the population.
Rev Med Electrón 39: 233-244.
32. del Prado GLG, Hernández CMG, Castillo MQ,
Hernández NG, Puig JF (2009) Characterization of oral health status and level
of knowledge in geriatric patients. Caricuao: Venezuela. Haban Cienc Rev Méd 8.
33. Rodriguez MD, Zárate E, Stewart K,
García-Vázquez JP, Ibarra EJE (2015) Ambient computing to support the
association of contextual cues with taking medication. Rev Mexican IngBioméd
36: 193-209.
-
 Table 1
Table 1 -
Table 2
-
Table 3
-
Table 4

QUICK LINKS
- SUBMIT MANUSCRIPT
- RECOMMEND THE JOURNAL
-
SUBSCRIBE FOR ALERTS
RELATED JOURNALS
- Journal of Pathology and Toxicology Research
- Journal of Allergy Research (ISSN:2642-326X)
- International Journal of Diabetes (ISSN: 2644-3031)
- Journal of Neurosurgery Imaging and Techniques (ISSN:2473-1943)
- International Journal of Medical and Clinical Imaging (ISSN:2573-1084)
- Journal of Otolaryngology and Neurotology Research(ISSN:2641-6956)
- Journal of Oral Health and Dentistry (ISSN: 2638-499X)


